

Join the inside story
Gain access to information about achondroplasia, including educational resources and upcoming events in your area. All sent directly to your inbox.
A deeper understanding of what comes after an achondroplasia diagnosis can help you move forward with confidence during this important time in your child’s development. Start by exploring local specialists.
Thinking about Raegan’s future in the beginning was scary, but now that I see her, I have no concerns.
Raechel, Mother of Raegan, 5 years old
Whether you’re learning about achondroplasia for the first time, know someone with the condition, or have it yourself, receiving your child’s diagnosis can initially feel overwhelming. However, confirming an achondroplasia diagnosis can allow you to start taking steps toward providing proactive and ongoing care for your child
For some parents, an achondroplasia diagnosis could be suspected prenatally from unexpected skeletal findings during routine pregnancy ultrasounds, typically around 26 weeks (end of the 2nd trimester), or if one or both parents have achondroplasia.
For other parents, an achondroplasia diagnosis may not be suspected for their child until after birth, when doctors may notice delayed growth, certain physical features, or smaller bones on X-rays.
To distinguish from other types of skeletal conditions, the genetic testing for achondroplasia will look specifically at the FGFR3 (fibroblast growth factor receptor 3) gene. FGFR3 is responsible for sending cell signals that slow bone growth—in achondroplasia, it slows bone growth more than it should.


For all children, bones only grow for a limited time—starting from before birth until late adolescence or early adulthood. In achondroplasia, the growth of bones that develop from cartilage (known as endochondral bones) is inhibited throughout the body.
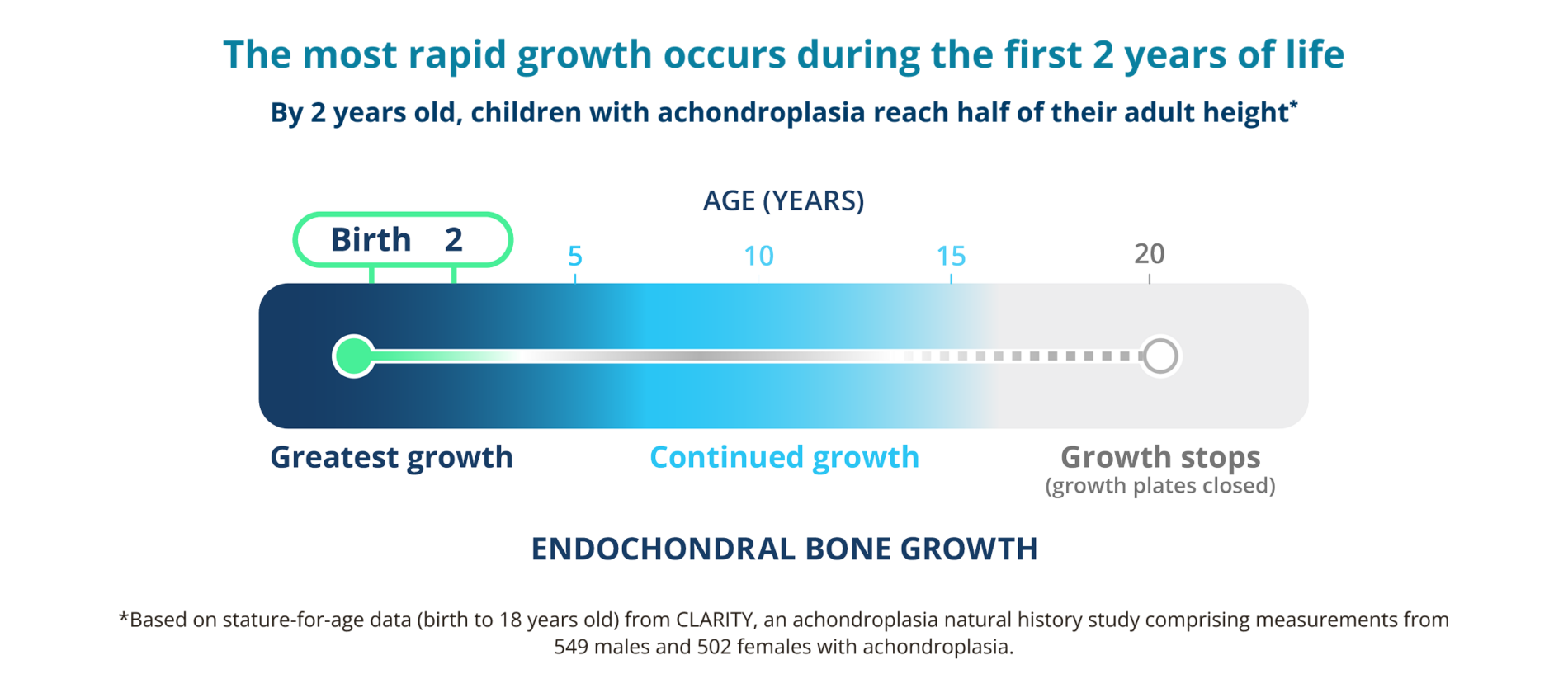

When bone growth is inhibited, parts of the skeleton becomes smaller, leaving less room in the body for some organs and nerves. This can impact your child’s health in different ways, such as difficulty breathing while asleep, having a smaller opening at the base of the skull, or repeat ear infections that can cause delays in motor or language development. All of which are more common in your child’s first 2 years of life and may benefit from early care.
Because achondroplasia is rare, it may be difficult to find doctors with the experience you need. Feel confident you’re finding specialized care for your child.
Locate healthcare providers in your area who have chosen to be part of the Achondroplasia Doctor Finder.
By using this website, you agree that:
After receiving an achondroplasia diagnosis, see how you can prepare to support your child throughout their journey and help ensure they receive the care they need at the right time.
Depending on your child’s unique medical needs, their care team will consist of different types of doctors, including a healthcare professional experienced in achondroplasia care (typically a geneticist or pediatric endocrinologist). Get a referral to a skeletal dysplasia center or experienced healthcare providers to get information about specialized care and treatment options.
Proactively schedule follow-up appointments with your healthcare team, along with special exams like a sleep study or hearing tests, especially during your child’s first 2 years of life. Appointments should occur at least every 2-4 months initially and then every 3-6 months depending on your child’s needs.
Share achondroplasia-specific growth charts and developmental guidelines with your care team and refer to them at each follow-up appointment. Your child may experience health effects that require a referral to relevant specialist like an ear, nose, and throat (ENT) doctor for ear infections, a pulmonologist for sleep breathing issues, or a pediatric neurologist for developmental delays.
Infants with achondroplasia need extra head, neck, and back support to ensure they are kept safe and have a healthy physical development. Learn how the potential impacts of achondroplasia could affect your child and see how you can help provide the correct physical adaptations.
Seek out support and resources from your care team and achondroplasia community to help your family throughout your journey—and don’t forget about taking care of yourself!

A foundation for proactive and ongoing care is a team effort. Healthcare professionals, members of the achondroplasia community, and the people closest to you all play an important role. You’re never alone as you navigate an achondroplasia diagnosis.
When Diego was born, Sela felt scared and had a lot of questions. With the help of an experienced care team and supportive community, she was able to feel more confident that she was providing her son with the best care.
Whether you’re expecting a child, have just welcomed one to your family, or are getting familiar with the new rhythms of life that come along with parenthood, an achondroplasia diagnosis can be an overwhelming time.
Find answers to common questions you may have about how to best support your child during this important time in their development.
Keep your infant’s head and neck upright to help avoid potential breathing problems, keep their full back (spine) straight and supported to help avoid curving, and help strengthen their core with supervised “tummy time.”
Movement and walking development may be affected by an enlarged head or bowed legs as your child grows. They may begin to move around in other ways, such as “snow plowing,” where they use their head as balancing support. These examples of creative movement demonstrate the ways your child is adapting to their body as they continue to learn to walk and move on their own terms. Encourage their progress and allow them to keep working through trips and stumbles on their way toward mobility.
It’s important to schedule regular check-ups with a doctor experienced in achondroplasia care. Together, you will continue monitoring your child’s growth and development using charts specifically made for children with achondroplasia.
Because your child may have difficulty supporting their head, use a solid-back high chair, infant seats, and strollers to support your child’s head and back to keep them safe and comfortable. It’s recommended to keep your child in a rear-facing car seat as long as possible and avoid automatic swings or other unsupported sitting devices.
Yes—however, you may need to work closely with staff and administrators to educate them about achondroplasia and how to best support your child’s unique needs, including necessary adaptions, health considerations, and other medical guidelines.
Discover a treatment option for infants and children with achondroplasia.

Gain access to information about achondroplasia, including educational resources and upcoming events in your area. All sent directly to your inbox.
References: